Patient Care Goals
Alleviate respiratory distress due to bronchospasm. Deliver appropriate therapy by differentiating other causes of respiratory distress.
Assessment
| Pediatric Pearls: | Signs & Symptoms: | Differential: |
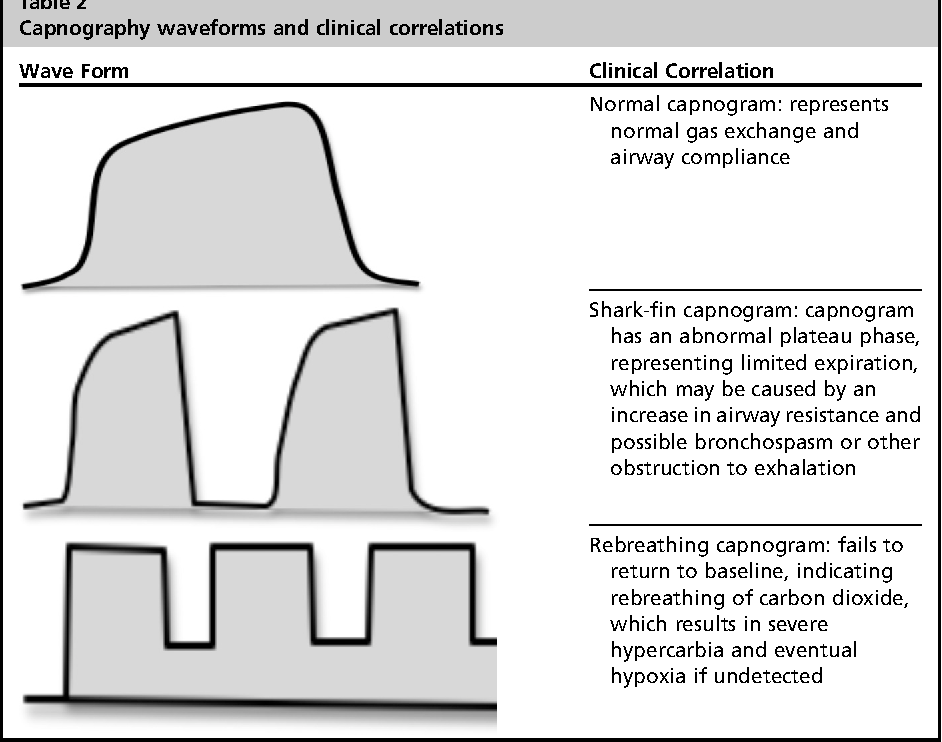
| □ Pediatric hypotension is defined as SBP < 70 + (age in years x 2) mmHg □ Wheezing in <2yo is often bronchiolitis and not asthma (unless they have a diagnosis of asthma). □ Work of breathing is important. Pediatric patients will not start to desaturate until they are in respiratory failure | □ Shortness of breath □ Pursed lip breathing □ Decreased ability to speak □ Increased respiratory rate and effort □ Wheezing, rhonchi, rales, stridor □ Use of accessory muscles □ Fever, cough □ Tachycardia □ Anxious appearance □ Shark-wave appearance on ETCO2 | □ Asthma / COPD (Emphysema, Bronchitis) □ Anaphylaxis □ Aspiration □ Pleural effusion □ Pneumonia □ Pulmonary embolus □ Pneumothorax □ Cardiac (MI or CHF) □ Pericardial tamponade □ Hyperventilation □ Inhaled toxin (CO, etc.) □ Croup / Epiglottitis □ Congenital heart disease Trauma □ Hydrocarbon ingestion |
Clinical Management Options
| EMT-B |
| • Oxygen target SpO2 92% – 96% • Blood Glucose Level Assessment • Basic Airway Management as needed |
| Paramedic |
| • Vascular access as appropriate for patient condition • Monitor and interpretation of ECG & EtCO2 • If wheezing (non-cardiac), consider Albuterol with Ipratropium • Dexamethasone • Consider early CPAP with PEEP in distressed patients • For severe bronchospasm, consider Magnesium Sulfate and/or IM epinephrine • Use caution in patient’s who are 65yo and older • Advance Airway Management as Needed |
Pearls
- EtCO2 and SpO2 must be monitored continuously if either are abnormal or decline in patient’s mental status/condition.
- Normalization of ETCO2 can mean improvement of the patient OR failure to compensate with impending death. Monitor the ETCO2 wave and mental status of the patient closely.
- Consider other reasons for respiratory distress such as pneumothorax or CHF (CHF can also wheeze, consider the entire patient history and exam).
- A silent chest in respiratory distress is a sign for pre-respiratory arrest.
- Chronic COPD may have elevated CO2 at baseline. Patient respiratory status must be reassessed after each nebulizer or medication administration to determine need for additional dosing.
- Chronic COPD may have lower O2 at baseline and have increased mortality with hyper-oxygenation. The O2 goal is above 90% (not 100%).
- Children less than 2yo are likely bronchiolitis, not asthma. Suctioning and oxygen is the first line treatment for bronchiolitis.
- A history of intubations and ICU stay can be a poor prognostic sign in some patients.
- Consider early CPAP in patients with respiratory distress.
- Magnesium may cause hypotension. Treat with fluid bolus.