| Assessment | ||
| Pediatric Pearls: | Signs & Symptoms: | Differential: |
| □ No transfusion for patient’s less than 10 years old □ Younger than 10 years old can suffer from too much volume that can cause respiratory failure □ Hypotension: (SBP < 70+ 2x Age in years) | □ Massive □ Hemorrhage □ diaphoresis □ AMS | □ Respiratory failure □Hypovolemia □ Trauma □ Tension pneumothorax |
Clinical Management Options
| EMT-B |
| •Control external hemorrhage and apply tourniquet(s) as necessary, including junctional tourniquets if needed and available. •Wound packing (junctional/extremity) with pressure dressing as appropriate and apply hemostatic gauze if available •BLS airway management •Keep patient supine and warm •Administer Oxygen via NRB to all serious hemorrhage patients. |
| Paramedic |
| •Vascular access For hemorrhagic shock, Tranexamic Acid and Calcium Chloride •Consider blood transfusion for the following: •Single SBP<70 OR •SBP < 90 with HR > 110 OR •ETCO2 < 25mmHg in patient that you are unable to obtain a blood pressure OR •Witnessed traumatic arrest after EMS arrival •Obtain VS every 10 minutes in patients receiving blood transfusion •If Hypotensive and no blood available, IV Crystalloid in 250 mL increments until MAP > 65 or SBP > 90 or until patient mentation improves •EKG monitoring •ETCO2 assessment •Advance airway management as needed |
Contact Medical Control as needed
Pearls
- Consider blood early in any patient that is hypotensive with evidence hemorrhage/blood loss
- Obtain verbal consent prior to transfusion if the patient is awake and alert. If the patient is not alert, then implied consent applies.
- If no blood available, consider permissive hypotension.
- In theory, permissive hypotension reduces the pressure on blood clots and therefore reduced bleeding. It is associated with improved survival in military data. It is reasonable to allow for lower blood pressure in patients who are mentating.
- An exclusion for permissive hypotension is evidence of brain trauma. Patient’s who are not mentating well do not have enough perfusion/volume and need volume.
- Consider staying on scene if time to blood is less than transport time, as this is also associated with improved survival.
- Severe bleeding from an extremity not rapidly controlled by direct pressure may necessitate the application of a tourniquet.
- Please obtain verbal consent in awake patients, especially young females. While the risk of allo-immunization (causes risk for miscarriage in Rh- mothers) is relatively low, it is not zero. That stated, our ultimate priority is saving the patient under our care.
- Consider other reasons for hypotension in patients who have experienced trauma (pneumothorax, spinal shock, etc).
- Pediatric Considerations:
- Pediatrics can be too small to handle to volume of blood for a full whole blood unit
- Patients who are 10 years old or 100 pounds can receive the full unit of blood without risk volume overload
- Trying to limit volume can be difficult, and pulling into a syringe can cause clots which are dangerous to the patients.
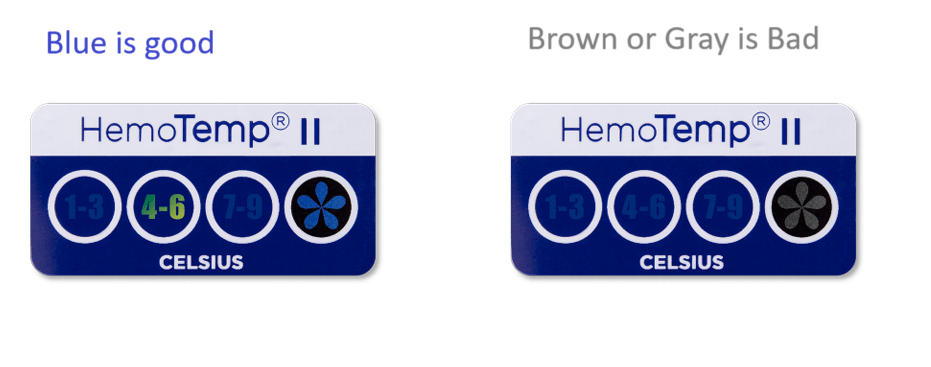
Visual Inspection of Blood